

Introduction: Follicular lymphoma (FL) is the most common indolent non-Hodgkin lymphoma subtype seen in Western countries. However, data on FL from Latin America (LATAM) are scarce. We aimed at better understanding the clinical features, treatment patterns and outcomes of patients with FL from LATAM.
Methods: This is a retrospective study that included all consecutive patients with a pathological diagnosis of FL at 18 participating centers from 12 LATAM countries. All cases were reviewed by specialized pathologists at their respective participating centers. Pertinent clinical, pathological and treatment data were collected. Responses were assessed per the Lugano criteria. Time to first treatment, progression-free survival after first treatment (PFS1) and overall survival (OS) were estimated using the Kaplan-Meier method.
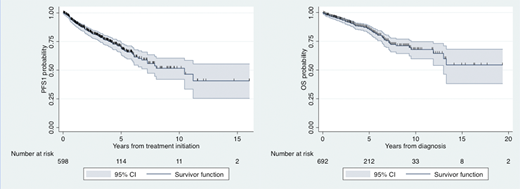
Results: A total of 763 patients were included in this analysis. On clinical features, 51% of patients were ≥60 years, 46% were male, 29% had extranodal involvement, 27% had bulky disease (≥6 cm in diameter), 68% had stage III/IV disease, 21% had hemoglobin <12 g/dl, 12% had serum albumin <3 g/dl, 34% had elevated serum LDH and 24% had B2-microglobulin ≥3,5 mg/l. Low, intermediate and high-risk FLIPI was seen in 43%, 33% and 23% of patients, respectively. Low, intermediate and high-risk FLIPI2 was seen in 18%, 64% and 17% of patients, respectively. The median time to first treatment was 0.08 years (95% CI 0.08-0.09), and 88% of patients started therapy within 1 year of diagnosis. Of the 647 treated patients, 70% received CHOP ± rituximab (R), 16% CVP ± R, 6% bendamustine ± R, 4% R alone and 4% other treatments. Response data were available in 628 patients with complete response in 72%, partial response in 21% and no response in 7%, for an overall response rate of 93%. The median PFS1 was 10.5 years (95% CI 7.3-not reached; Figure), and 74 patients (12%) had disease progression within 24 months of first treatment initiation (POD24). The median OS was 21.1 years (95% CI 13-not reached; Figure). Patients with low, intermediate and high FLIPI had median OS not reached, 21.1 and 9.5 years, respectively (p<0.001). Patients with low, intermediate and high FLIPI2 had median OS not reached, 21.1 and 6.8 years, respectively (p<0.001). Patients who had and did not have POD24 had median OS of 7.3 years (95% CI 4.8-not reached) and 21.1 years (95% CI 13-not reached), respectively (p<0.001).
Conclusion: This large, real world evidence LATAM cohort of 763 patients with FL showed a higher than expected female incidence as well as higher rates of extranodal and bulky disease than previously reported in Western cohorts. Chemoimmunotherapy is the standard approach to FL patients in LATAM, which is associated with high rates of response and highly encouraging PFS and OS rates. Our study validates the prognostic value of FLIPI, FLIPI2 and POD24.
Villela:Roche: Other: advisory board, Speakers Bureau; amgen: Speakers Bureau. Peña:Amgen: Speakers Bureau; BindingSite: Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Sandoz: Membership on an entity's Board of Directors or advisory committees; Roche: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees. Idrobo:Takeda: Honoraria, Speakers Bureau; Amgen: Honoraria, Speakers Bureau; Tecnofarma: Honoraria, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; Abbvie: Honoraria, Speakers Bureau. Abello:Dr. Reddy's: Consultancy, Research Funding; Takeda: Honoraria, Research Funding; Novartis: Consultancy, Honoraria; Amgen: Consultancy, Research Funding; Abbvie: Consultancy, Research Funding. Perini:AbbVie, Janssen: Speakers Bureau; Janssen, Takeda: Honoraria. Castillo:Abbvie: Research Funding; Janssen: Consultancy, Research Funding; Kymera: Consultancy; TG Therapeutics: Research Funding; Beigene: Consultancy, Research Funding; Pharmacyclics: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal